|
|
|
|
|
||
| SEARCH | SUBSCRIBE | ||
|
Stakes
high to help those with chronic diseases By Sandi
Doughton, the
Lois Stolle, 61, follows the movements of physical-therapy aide Tem Haile in a session at Providence ElderPlace, a program that provides comprehensive care for 176 people age 55 and older in Seattle Not
even 60 years old, the "I
woke up screaming: 'Get me out of here!' " recalled Stolle, whose
mother languished in a nursing home for two decades after a series of
strokes. "I didn't want the same thing to happen to me." Society
doesn't want it, either. On
the cusp of an unprecedented age boom, "The
stakes are really quite high," said Dr. Ed Wagner, director of Group
Health Cooperative's W.A. MacColl Institute for Healthcare Innovation.
Wagner
and his colleagues are at the forefront of a national movement to help
people like Stolle — who suffer from incurable, long-term diseases —
stay healthier as they age. Called the chronic-care model, it sounds like
nothing more than common sense: Keep diabetes, high blood pressure, heart
disease, asthma and other chronic conditions under control before they
spiral into crippling complications that are costly to treat and rob so
many of their vitality and independence. "Don't
spend the last 15 years of your life blind, or as an amputee, because your
diabetes wasn't managed properly. Don't die young from congestive heart
failure, because it wasn't managed properly," said health-care
consultant John Fiorillo, author of a Robert Wood Johnson Foundation
report on chronic illness in But
few seniors today get the coordinated care required to control chronic
diseases, which primarily afflict the elderly — and consume 75 percent
of the national health-care budget. "We
have a health-care system that's pretty good if you have an acute problem,
like a broken arm or pneumonia," Wagner said. "But it's not set
up to deal with these lifelong illnesses." More
than half of the people who suffer from chronic diseases are not getting
the tests and treatments that are considered state-of-the-art medical
care, he said. A 70-year-old with multiple health problems may bounce
between four or five specialists, who never confer with each other. The
patient is left with a bewildering array of drugs, conflicting advice and
little real guidance. The
costs — both in dollars and quality of life — are already staggering
and are certain to escalate as the number of Americans 65 and older
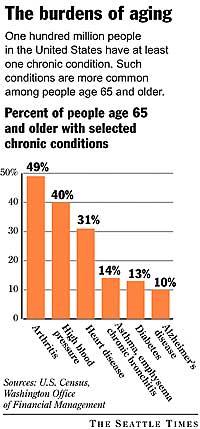
doubles by 2030, Wagner said. More
than 80 percent of seniors suffer from at least one chronic ailment, and
25 percent have four or more. For
diabetes, that translates into a cost of more than $32 billion a year.
Without improvements in health care, analysts project the total medical
bill for the nation's elderly will at least double, and possibly
quadruple, over the next few decades, conceivably reaching $1.3 trillion a
year by 2020. Better
care, lower cost Stolle's
experience is testament to the power of coordinated health care to reduce
human misery while also saving money. Now
61, she's back in her own apartment. Every morning, a home-health aide
helps her check her blood sugar and take the proper dose of insulin, along
with nine other drugs for everything from high blood pressure to bloating.
Twice
a week, she shuttles to an adult day center in Because
of the physical therapy she receives at the center, Stolle can walk short
distances with a walker. She has lost nearly 75 pounds, thanks largely to
the dietitian who helps plan her menus and the healthful meals served at
the center. She gets regular physical exams from the program's in-house
geriatrician, Dr. Assad Kazemi.
A
pharmacist sorts Stolle's medications into a pill organizer, with separate
compartments for each day's dosages. Podiatrists and eye doctors visit the
center to check for diabetic foot sores, which could lead to amputation if
not treated early, and vision problems that could progress to blindness
without early intervention. If staffers notice that Stolle seems to be
dragging, they'll alert Kazemi to do a quick evaluation. "We
know everyone's history and background here," he said. "We don't
wait for things to get so bad that people wind up in the hospital." For
Stolle, the most tangible benefits are being able to live on her own
again, and feeling well enough to socialize with her sister and
girlfriends. "I'm
so much better since I've been here," she said. For
Medicare and Medicaid, the federal and state programs that pay for the
ElderPlace program, the benefit is a savings of up to 15 percent compared
with what it would cost to keep Stolle in a nursing home. Prevention
is key In
the traditional approach to medicine, people with chronic diseases usually
visit the doctor only when there's a specific problem. Someone with heart
disease might come in complaining of fluid retention and painfully swollen
legs. An asthmatic might go to the emergency room when he can't breathe.
The
doctor deals with the crisis at hand but has little time to address the
underlying reasons the disease is out of control. She might admonish the
patient to lose weight and hand over a pamphlet on exercise. Then,
three months later, the patient is back, with the same problems — or
worse. "It's
frustrating for everyone," Wagner said. Chronic
care turns the system upside down, placing the emphasis on regularly
scheduled checkups. Nurses call patients at home to see if they're taking
their medications or eating properly. Doctors use computer programs to
identify patients with specific conditions and to see, at a glance, their
treatment histories. That also helps to ensure each patient receives all
the recommended tests and the most effective medications. "I
don't have to spend my time flipping through all the sheets of paper in
the chart," said Dr. Kevin Martin, an Martin
can document that diabetes patients at his largely middle-class practice
are better at keeping their blood sugar under control and are getting more
regular eye checkups, cholesterol screenings and other follow-ups. Financially,
the new approach is a wash. "I
can't say that I'm getting paid any better," Martin said. "My
own belief is that it makes us more efficient; we're giving better care,
and it makes the patients happier." Keeping
patients happy and being aware of what else is going on in their lives is
crucial, because people who live with lifelong diseases must take the lead
in managing their health. Under
the chronic-care model, doctors, nurses and educators work with patients
to figure out what's keeping them from taking their drugs regularly,
losing weight or eating healthfully. The team then works to remove those
barriers and helps the patient set achievable goals. At
Highpoint Medical Clinic, a low-income clinic in "They
quickly realize: If I eat a bag of Lay's potato chips, my blood pressure
is going to be higher," Baird said. "That has much more of an
impact than me wagging my finger at them and saying: 'You need to lose 10
pounds.' " Baird
often schedules diabetic patients for group visits, where everyone gets
their eyes, feet and blood sugar checked, while sharing health tips and
learning more about the condition they all share. Social workers,
dietitians, nurses and doctors work together to coordinate each patient's
care. "Everybody
talks to everybody else," said Jayne Nelson, a clinic patient who
lives in Under
Baird's guidance, Nelson gave up the weekend drinking parties that
aggravated her diabetes and can control the condition with diet alone. She
exercises and keeps careful records of her blood sugar. "They
make me feel like it's worth taking care of myself," Nelson said. And
at the age of 41, Nelson understands that managing chronic disease isn't
only important for the elderly. "If
you want to prolong your life, you've got to do things differently,"
she said. A
slow change As
leaders of a national program of the Robert Wood Johnson Foundation called
"Improving Chronic Illness Care," Wagner and his colleagues have
trained more than 1,000 doctors, medical groups and clinic staffs across
the country in the chronic-care model. The Washington Department of Health
also is spreading the word through an award-winning program focused on
diabetes. Even
the state's poorest residents are benefiting from a scaled-down version of
chronic care. More than 27,000 Medicaid patients with asthma, kidney
disease, diabetes and heart disease get regular calls from a network of
contract nurses who check their status, remind them to take medications
and answer questions. Health
officials estimate that the program already has saved the state $2 million
as a result of reduced hospitalizations and fewer costly complications. Other
success stories are starting to accumulate. At
Group Health in Though
it often requires more work and money up front to change systems and
adjust to a new way of working, doctors who have embraced the model are
uniformly enthusiastic. Most also believe the new approach is more
cost-efficient and engenders patient loyalty. "I
firmly believe the better you take care of people, the cheaper it is in
the long run," Baird said. But
many obstacles remain, particularly the traditional payment system used by
most insurance companies and Medicare, the program that pays for most
seniors' health care. Medical practices usually don't get reimbursed for
patient education, a mainstay of chronic-care systems, nor do many
insurers cover phone consultations by nurses or blood-pressure monitors
and other home equipment for patients, Wagner said. The
Medicare reforms being debated in Congress offer few incentives to promote
chronic care. But as the shadow of the coming age wave stretches across
the country, policymakers soon might be overwhelmed by the sheer numbers
— and the growing discontent of the millions of Americans who want to
age well, despite their chronic illnesses. "The way we deal with the chronic patient and the chronic elderly patient is the bellwether for our health system," said Fiorillo, the health-care consultant. "If the system can't deal with the chronically ill by providing high-quality, affordable care, the system is not going to succeed." Copyright
© 2002 Global Action on Aging |
||||||||||||||