Atrial
fibrillation: strategies to control, combat, and cure
By: Robert W. Griffith, MD
Health and Age, July 26, 2002
.
Introduction
Normally the heart beats regularly; when one's
resting, it's a little slower or faster, according to the respiration --
this is called 'sinus rhythm'. Atrial fibrillation (AF) is the commonest
heart 'arrhythmia', or irregular heartbeat. It's a very irregular and fast
heart rhythm involving the upper chambers (atria) of the heart.
AF is more common as people get older, but it's also
being seen increasingly often, irrespective of age. It can occur in
otherwise healthy people without any obvious cause. More often, however,
it is seen in people with high blood pressure, heart disease, diabetes, an
overactive thyroid, or who drink too much alcohol.
Today, more than 5% of those over 65 have AF. It's
commoner in men, and men who have had a heart attack (myocardial
infarction, or MI) are at especial risk. Rarely, AF runs in families.
The big threat of AF is an increased likelihood of
stroke; a stroke may occur in 1% to 2% of patients in their 50s, and in
20% of those in their 80s. Mortality rates in people with AF are double
the norm, due to stroke, heart failure, or MI.
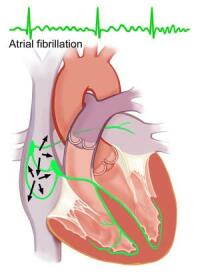
What happens in atrial fibrillation?
Normally, the natural pacemaker of the heart situated
in the atria sends an electrical signal to the rest of the heart, causing
the whole heart -- both atria and ventricles - to contract. During AF, the
atria beat very rapidly and out of rhythm with the rest of the heart; this
interferes with the overall pumping action of the heart.
The irregular fast rhythm of AF arises from one or
more abnormal pacemakers, or 'excitable foci', that are often situated
just inside the pulmonary veins as they enter the atria; occasionally the
foci may be in the nearby part of the superior vena cava (the great vein
draining the upper body). How a focus is triggered, and what triggers it,
is still unclear.
In AF, the period of time after an electrical signal
during which the tissues cannot be stimulated again (the 'refractory
period') is shorter than normal. This allows more frequent, irregular
waves of contraction in the atria. The atria adapt to this by
progressively shortening their refractory periods, leading to the adage
"atrial fibrillation begets atrial fibrillation" -- i.e. left
alone, the condition tends to worsen.
With the atria failing to contract properly, blood
can pool, or move very slowly ('stasis'). This is most marked in the left
atrium, where a clot (or 'thrombus') can form, bits of which can, at any
time, enter the blood stream and block a small brain artery -- thus
causing a stoke.
The types of AF
A first episode of AF is called 'acute atrial
fibrillation'. Subsequent episodes are called 'recurrent'. If the episodes
stop on their own, they're termed 'paroxysmal'.
If the episodes are so frequent or long-lasting that
the physician needs to stop them (this is called cardioversion), it's
'persistent AF'. And if they cannot be stopped by cardioversion, or if
they have lasted a year without such an attempt, AF is regarded as
'permanent'.
When it's known that the fibrillation originates at
one or more foci in an otherwise normal heart, it's called 'focal AF'.
This type (which may be paroxysmal or permanent) is commoner in patients
in their 50s and 60s, and is three times
more frequent in men.
Symptoms and diagnosis of AF
Some people will have no symptoms; others will have
some shortness of breath, and a feeling of palpitations or fluttering in
their chest. Fainting can occur, and there can be chest pain.
AF is diagnosed from the history, a clinical exam,
and an electrocardiogram (ECG). Wearing a heart monitor (a Holter monitor)
for a period can help detect paroxysmal AF if there are no symptoms to go
on. Doctors will often order an echocardiogram, to look for changes in the
size and functioning of the 4 heart chambers.
Treatment
First, the heart rate must be slowed to a more normal
rate. This will usually decrease symptoms. Calcium-channel blocking drugs
(e.g. diltiazem, verapamil) or beta-blockers (e.g. sotolol) are used for
this.
To prevent the formation of thrombi in the left
atrium, a blood thinner, or anticoagulant, should be given; warfarin is
the usual choice. This is important if AF has existed for more than 48
hours and an attempt to restore normal (sinus) rhythm is planned. In case
of doubt, a special exam (trans-esophageal echocardiography) can detect
the presence of atrial thrombi.
Re-establishing sinus rhythm (called 'cardioversion')
can be done using medication, or by an electrical shock. There are various
types of drugs called antiarrhythmics that are intended to stop heartbeat
irregularities. Those used for medical cardioversion include flecainide
and amiodarone. As they may have serious side effects, medical
cardioversion must be done in hospital.
Electrical cardioversion can be 'external' or
'internal'. External cardioversion involves using electric paddles applied
to the chest wall, under general anesthesia. The shock halts the abnormal
fast pacemaker and allows the normal pacemaker of the heart to take over.
Success rates range from 65% to 90%. If this doesn't restore normal
rhythm, the patient can be given an antiarrhythmic drug for a short
period, and the procedure repeated.
Internal electrical cardioversion involves having
small tubes that carry electric wires passed under the skin to deliver
shocks at specific sites in the heart (usually in the right atrium); this
is done under general anesthesia. Using this technique, normal rhythm is
restored in 90% of those cases where external cardioversion has failed.
Once normal rhythm has been achieved, it must be
maintained. Sotalol, flecainide, propafenone, and amiodarone are all
effective medications for suppressing paroxysms of AF. In some cases,
surgery is done to implant an atrial pacemaker. (This is different from
the usual pacemaker, which regulates the ventricular beats.) Atrial pacing
is effective; it suppresses the undesired focal beats and improves
electrical conduction.
It's also possible, using an approach similar to
internal cardioversion, to detect the site of abnormal foci and then
destroy them by radio-frequency energy delivered along the wires. In
patients with only one abnormal focus, success rates are near 90%, but
this falls to about 50% in those with three or more foci.
Finally, a surgical procedure, the Maze operation,
involves cutting the atria into segments and then rejoining them. It
reduces the amount of atrial tissue available for fibrillation to 'breed'.
Success rates are high, but the procedure is quite risky.
Preventing stroke
Should people with AF be on long-term anticoagulants?
It's a matter of balancing the risk of side effects (chiefly hemorrhage)
against the risk of having a stroke. Someone with AF is at greatly
increased risk of stroke if they are over 65, have had a previous stoke or
transient ischemic attacks (TIAs), have diabetes, high blood pressure, or
heart failure. It's been shown that anticoagulation using warfarin reduces
the risk of thrombotic stroke in AF patients by 68%, and cuts mortality by
33%. Aspirin is much less effective than warfarin.
Conclusions
The management of AF has improved in recent years, so
that more attention is being paid these days to ways of curing it, rather
than suppressing paroxysms or future episodes. For those patients who
cannot be cured, suitable medications and procedures, as well as
anticoagulant therapy, can go a long way to making life quite tolerable
and less hazardous.
Source
Atrial
fibrillation: strategies to control, combat, and cure. NS. Peters,
RJ. Schilling, P. Kanagaratnam, et al., Lancet, 2002, vol. 359,
pp. 593--603


